This article is general information for our patients, not a diagnosis. If something in your mouth hurts, changes, or worries you, have it examined.
Drafted with AI assistance and reviewed for accuracy by Dr. Nick Jadidi.
A jaw that aches in front of the ear, clicks when you chew, or feels tight first thing in the morning is something people bring to me most weeks, and usually nothing serious is wrong. Around one in three people run into jaw trouble at some point, and roughly one in ten adults (5–12%) has it at any given time. It’s about twice as common in women, and most often shows up between the ages of 20 and 40.
One point up front: none of the clues below is a diagnosis on its own. A sore chewing muscle, a strained joint, and a back tooth throwing pain toward the ear can all feel much the same from the outside, so pain that feels like it’s coming from the muscle can just as easily be the joint or the tooth. Sorting the three apart takes what you describe, a hands-on exam of the joint and chewing muscles, how each responds when I test it, and an X-ray in the cases that call for one. That’s a call I make with you in the room, not one you can settle from a symptom list.
What is TMJ, and what actually causes jaw pain?
The TMJ (temporomandibular joint) is the jaw joint just in front of each ear. It hinges, then slides forward out of its socket to open wide, with a small disc of firm cartilage cushioning the bones. TMD (temporomandibular disorder) is the umbrella term for the problems that make it hurt, click or stiffen: not one disease but a few patterns, often more than one at once.
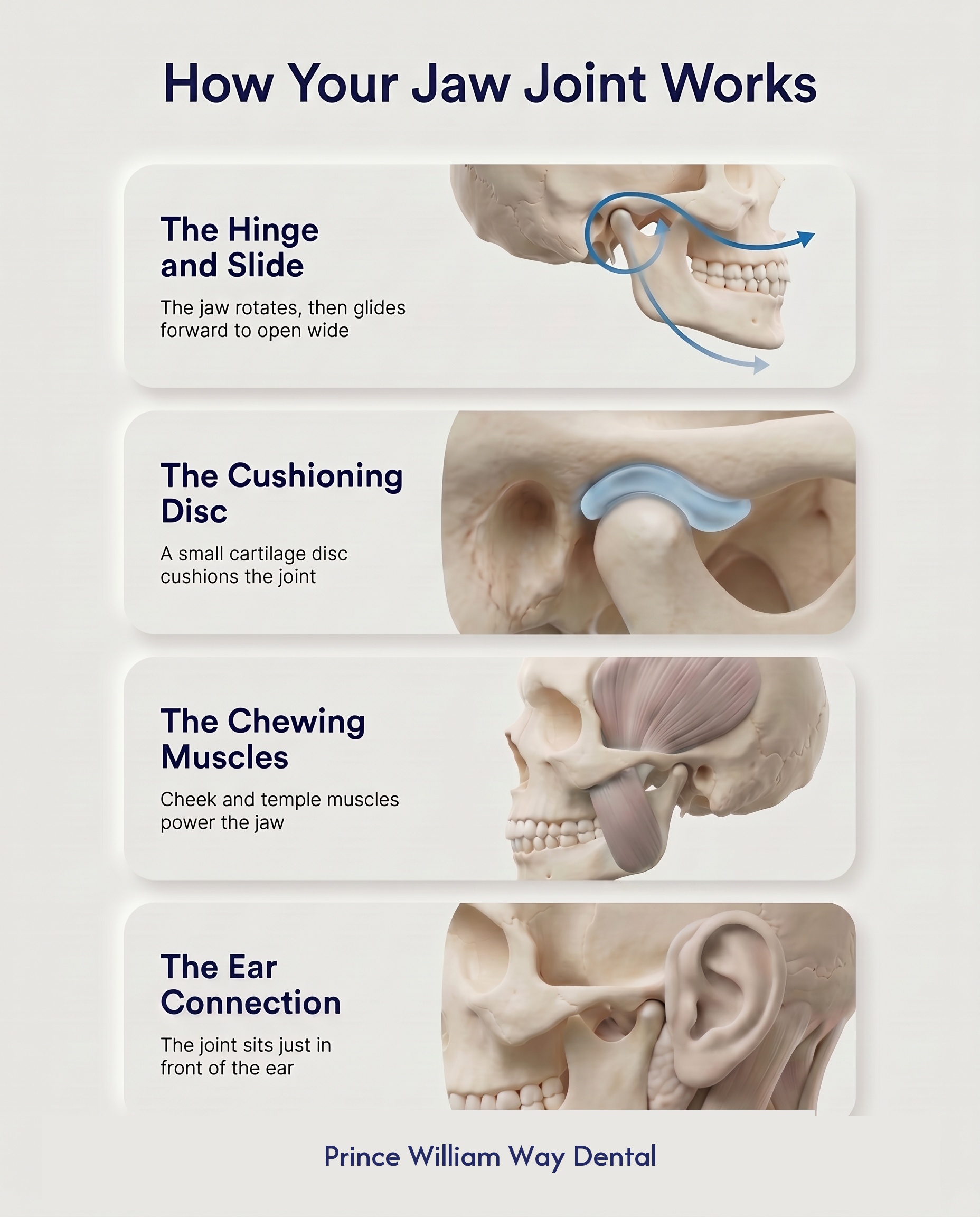
- Muscle pain — by far the most common: the chewing muscles in the cheek and temple get overworked and achy.
- A slipped cushion (disc displacement) — the disc slips out of position, which tends to cause clicking and, less often, catching or locking.
- Joint wear — wear-and-tear arthritis inside the joint, tending toward a grating feel and morning stiffness, more often with age.
Which pattern matters, because the muscle type (the one most people have) usually responds well to rest and simple care.
Why does my jaw and ear hurt on one side?
Jaw pain is often felt in one ear because the jaw joint sits millimetres from the ear canal and shares nerves with it — pain that gets worse when you chew, yawn or talk points to the jaw, not the ear. That’s why many people chase an ear problem for weeks first, especially when a doctor has already looked and found the ear itself healthy. The pain can also travel to the temple, down the jawline to the neck, or toward the back teeth, sometimes with fullness or ringing. Even so, how the pain behaves is a pointer, not proof.
| Clue | Points toward the jaw (TMD) | Points toward an ear infection |
|---|---|---|
| Chewing, yawning, long talking | Tends to make it worse | Makes little difference |
| Hearing | Usually normal; sometimes fullness or ringing | Often muffled or reduced |
| Fever or discharge from the ear | Usually absent | Common |
| A doctor’s look in the ear | Healthy ear | Inflamed eardrum or canal |
What triggers a TMJ / jaw-pain flare?
TMD is usually an overload problem, not a single injury: flares happen when several things stack up past what the joint and muscles tolerate.
- Clenching and grinding (bruxism) — the big one: hours of unconscious muscle work, asleep or at a screen, leave the chewing muscles aching. There’s more on the morning pattern below.
- Stress — raises muscle tension and lowers your pain threshold at once, so flares often land during exams, deadlines or hard stretches.
- Extra chewing hours — gum, nails, pens and ice add load the joint was never budgeted for.
- Sustained wide opening — a long dental appointment or wisdom tooth removal can set off a temporary flare that usually settles within two to a few weeks.
- Posture — a forward-head desk position keeps neck and jaw muscles working overtime; neck and jaw pain are frequent companions.
Less often a blow to the jaw, whiplash, very flexible joints or a wider joint condition like rheumatoid arthritis play a part. That’s part of why I take a proper history rather than assume.
Why does my jaw feel tight first thing in the morning?
A jaw that feels tight or achy when you wake usually means the chewing muscles have been working overnight — night-time clenching and grinding (bruxism) is the most common reason for morning jaw tightness. The clues tend to travel together: flattened or chipped tooth edges, a cheek or temple ache that fades as the day goes on, and sometimes a partner who hears the grinding at night. Daytime counts too: plenty of people catch their teeth pressed together at a screen without noticing, and the teeth-apart habit in the home routine below is how you break it. If mornings are reliably your worst time, mention it when you call, because that pattern shapes the plan, including whether a night guard is worth considering.
Is it bad if my jaw clicks but doesn’t hurt?
A jaw that clicks but doesn’t hurt or lock is usually a harmless mechanical quirk, not a disease to fix — just the jawbone popping over a slightly out-of-place disc as it opens and closes. Plenty of people click for years with no pain and no consequences, and a click alone wouldn’t even send me to an X-ray. Another reassuring tell is which way the jaw drifts as you open: if it swings to one side but straightens out by the time your mouth is fully open, that’s usually the harmless kind; a jaw that stays pulled to one side and won’t open far is the one to have looked at.
What earns a closer look is a click that turns painful, or a jaw that starts to catch or stick on the way open. If it catches, don’t force it: relax, place both thumbs on your lower back teeth, gently wiggle the jaw from side to side to loosen it, then ease it back and forward to free it. Catching that’s getting more frequent, or a jaw that has stopped clicking and now won’t open as far, can mean the disc is staying out of position, and is worth examining.
How do I relieve TMJ jaw pain at home?
Treat a flared jaw like a sprained ankle — protect it and let it settle: soft food, moist heat, gentle massage, teeth apart and no gum for two weeks settles most flares. Around 70–80% of TMD improves substantially with simple, non-surgical care within three to six months, and much of that is in your hands: expect clear easing inside two weeks, with full settling sometimes taking that full three-to-six-month window.
| What to do | How | Why it helps |
|---|---|---|
| Soft-diet stint | Pasta, eggs, fish, soups for a week or two; cut food small | Lowers the daily workload so tired muscles recover |
| Moist heat | Warm, wet facecloth on cheek and temple, 10-15 minutes, a few times a day | Relaxes muscle, improves blood flow |
| Massage and gentle exercises | Slow circles on the cheek muscle; then, tongue on the roof of the mouth, open slowly to just before discomfort, hold a moment, a few repeats | Releases tension, keeps the joint moving |
| Teeth apart, lips together | Teeth touch only when you’re eating | Breaks the daytime clenching habit |
| Drop the extra chewing | No gum, nails, pens or ice for now | Removes load the joint doesn’t need |
| Supported yawning | A fist gently under the chin as a yawn comes | Stops a sore joint opening too wide |
| Ease the soreness | An over-the-counter anti-inflammatory painkiller, with food, short-term if it’s safe for you | Calms inflammation in muscle and joint |
A pharmacist can tell you which painkiller suits you and how much, which matters if you take anything else regularly or manage a health condition. Give it a full two weeks; most flares respond. If yours doesn’t, or keeps coming back, that’s when an exam earns its keep.
Do night guards actually help?
Night guards often help when grinding or clenching is driving the pain — many people improve, though some notice little change if daytime habits or stress are the real driver. A night guard (an occlusal splint) is a precisely fitted hard cover, usually for the upper teeth, worn while you sleep.

I’ll be straight, because guards are sometimes oversold. What one reliably does is protect the teeth: grinding can wear, chip and crack them, and the guard takes that damage instead. Pain relief is less predictable: it helps most when night-time grinding is clearly the driver, and a night-only appliance can’t reach the daytime habits or stress that keep some jaws sore. So I pair a guard with the self-care above and review after two to four weeks; if grinding is part of your picture, it’s worth reading how grinding and clenching damage teeth, and what we do about it. One thing we deliberately don’t do is grind down healthy teeth to treat TMD: the idea that a slightly-off bite causes most jaw pain hasn’t held up, and reshaping teeth can’t be undone.
What we do when you come in
An assessment here is mostly careful listening and a hands-on exam. I ask about the pain pattern, sleep, stress, habits and health, then measure how far you open (around 40 mm, about three finger-widths, is typical), watch whether the jaw tracks straight, feel the joint and muscles for tenderness, and listen for clicking versus grating. I look hard at the teeth too, because a cracked or inflamed back tooth can throw pain toward the joint and imitate TMD convincingly. X-rays come in only when they’d change the plan: suspected joint wear, or after an injury.
None of those steps stands alone: it’s how the joint, muscle, and tooth findings line up, alongside what you’ve told me, that points to an answer, and only in the chair. Treatment then climbs from the gentlest rungs: the self-care routine, short-term anti-inflammatory relief, a night guard where grinding is involved, and jaw and neck physiotherapy (good evidence behind it). If pain runs past about three months despite that, if opening stays very limited (below about 25 mm, under two finger-widths), or if anything unusual turns up, I refer you to a jaw surgeon (oral and maxillofacial surgeon) or a facial-pain specialist.
When is jaw pain a sign of something serious?
Most jaw pain isn’t a sign of anything serious and can wait for a routine visit; the exceptions below are the ones I want examined promptly.
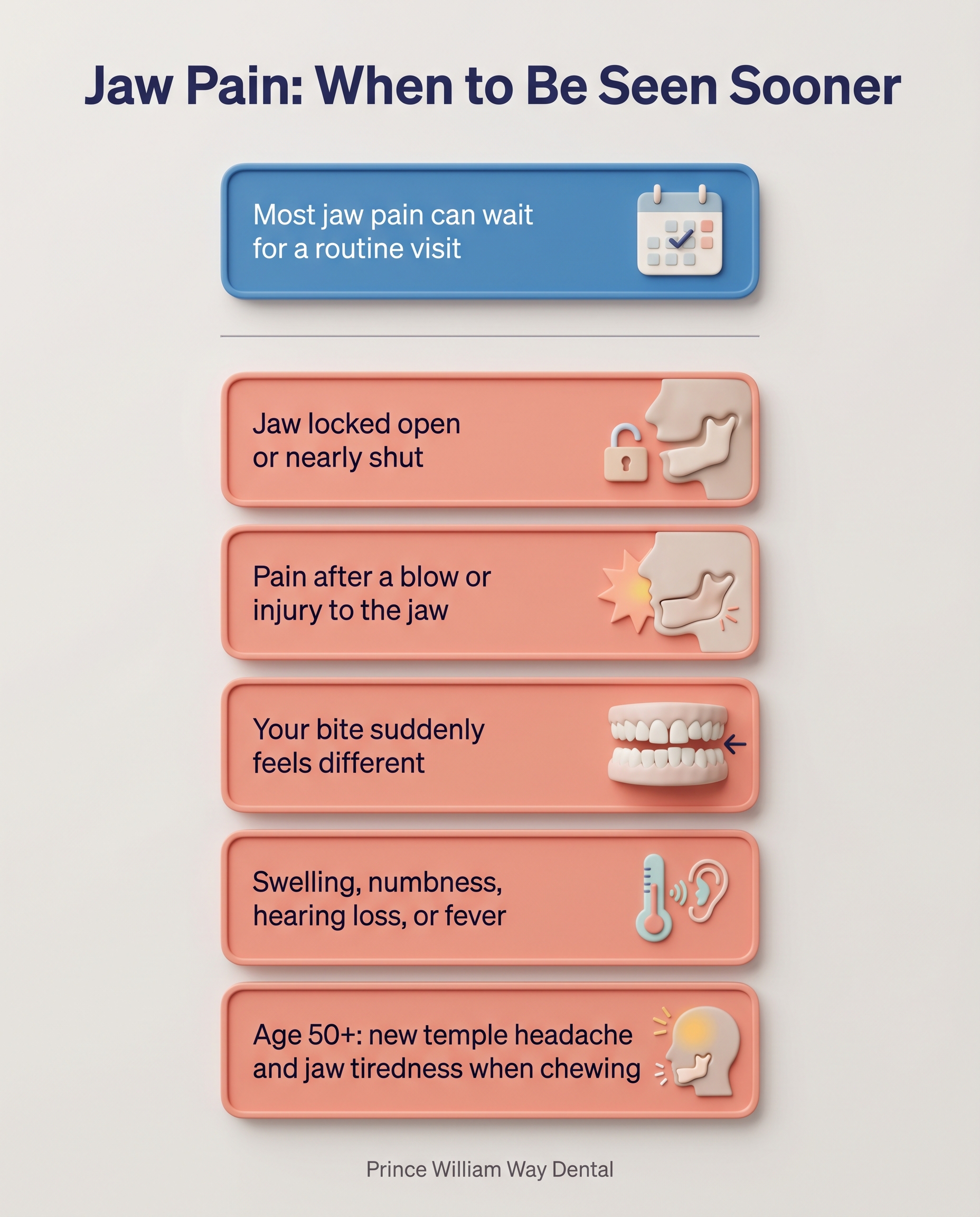
- A locked jaw — stuck nearly shut and unable to open, or stuck open and unable to close. It should be seen as soon as we can, through our emergency dental care in Barrie.
- Jaw pain after an injury — a fall, a sports impact, a blow all need checking for a break.
- A bite that’s changing — teeth that suddenly don’t meet the way they used to can mean something is shifting in the joint.
- Change that keeps worsening — opening that keeps shrinking, swelling over the joint, facial numbness or weakness, or new one-sided hearing or balance trouble.
- Over 50 with a new temple headache plus a jaw that cramps or tires after a few minutes of chewing: see a doctor straight away. This can point to an inflamed blood-vessel condition (giant cell arteritis) that’s treatable but won’t wait.
- Fever with facial swelling points toward infection rather than TMD, and shouldn’t wait either.
Each is uncommon, but the reassurance about ordinary jaw pain only holds once they’re ruled out.
Will I need surgery?
Almost certainly not — around 70–80% of TMD improves substantially with simple, non-surgical care within three to six months, and surgery isn’t on the table for the typical aching-muscle, clicking-joint jaw. Surgery has a place: joints damaged by serious arthritis, a disc that stays stuck despite months of proper non-surgical care, or repeated full dislocations. The usual procedure is a specialist wash-out through two small needles (arthrocentesis), which helps roughly 70–80% of carefully chosen cases at six to twelve months. Open joint surgery is rare. Most people who stick with the simple, reversible care above never need more.
This guide is part of our Adult Patient Information library. If your jaw has been bothering you, we’re happy to take a proper look: call Prince William Way Dental at 705-721-9229 or book online — online booking covers new patient visits and emergency examinations. For anything else, reach us through our contact page. We’ll start with the simplest care that works.
